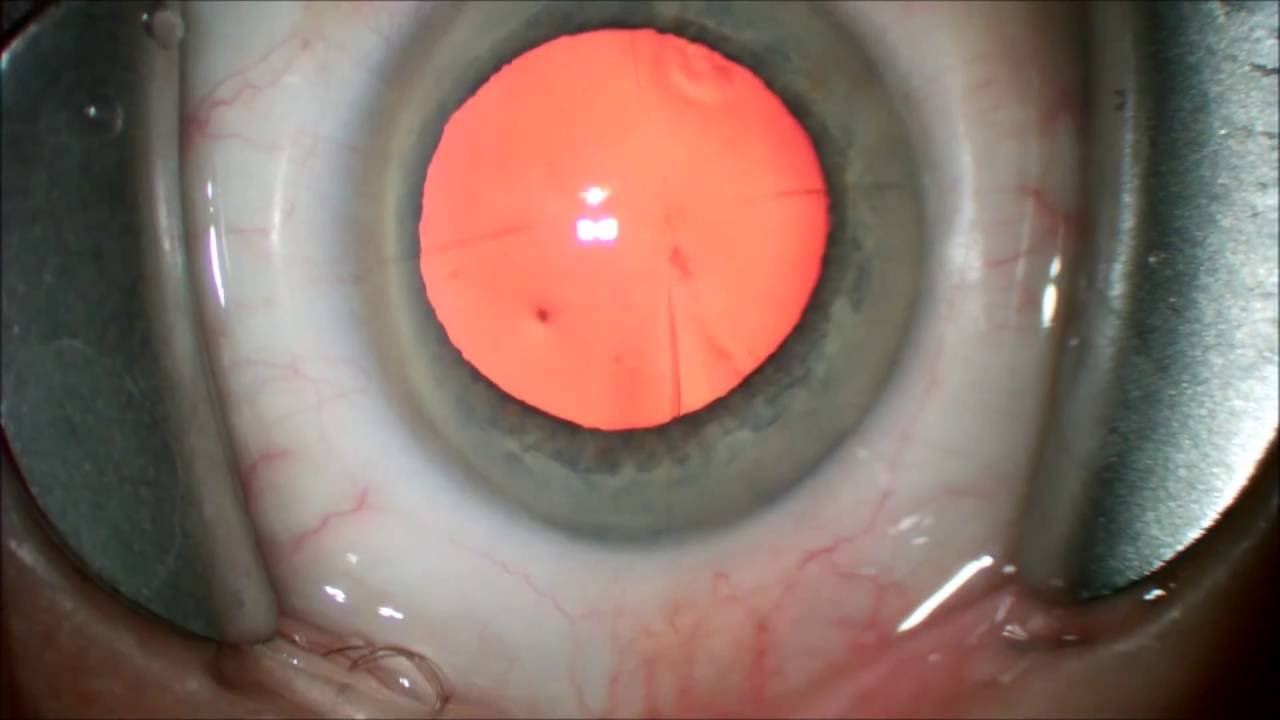
Radial Keratotomy was popularized by Dr. Fyodorov in the 80's and early 90's as a surgical correction of refractive errors, it involved making radial and circumferential incisions in the clear cornea up to 90% depth with a diamond blade. As many as 32 incisions were placed.
This obviously poses a challenge to cataract surgeons many years later. The challenges are both in intra-ocular lens calculations and performing the surgery in the previously operated eyes.
Surgical tips:
1)Avoid RK (radial keratotomy) incisions, leave as large a margin of untouched tissue next to all incisions, if this is not possible make scleral tunnel incisions.
2)Avoid over torquing or stretching incisions, this will sometimes break open adjacent RK incisions.
3)If RK incisions open suture perpendicular to opened rk incisions, self sealing wounds will still be self sealing with intact roof of incision. Use Resure sealant if still leaking after placing sutures, at end of case. D1 postoperative leaks, can be tamponaded with bandage contact lenses in some cases.
Dr. Kavanagh practices at Eye Associates of South Texas with offices in: Seguin, San Antonio, New Braunfels, Luling, Gonzales and Hondo. 830-379-3937. www.eyeassociatesofsouthtexas.com or www.eyestx.com
Dr. Kavanagh is fellowship trained in Glaucoma.
Dr. Kavanagh is a board certified ophthalmologist and clinical assistant professor at University of Texas Health Science Center in San Antonio Texas, where he has taught many residents cataract and glaucoma surgery. Dr. Kavanagh has performed over 10,000 cataract procedures with intraocular lens implantation. He implants: Restor, Technis Multi Focal (MF), Crystalens, Toric IOLs.






















































![Gaming Phones Evolution [2003-2021]](https://i.ytimg.com/vi/hfABAtBcRuY/mqdefault.jpg)

















